




The evaluation of skin temperature variability within the lower
extremities after bio-theramal inserts application
Małgorzata Łukowicz, Magdalena Weber-Zimmermann, Katarzyna Ciechanowska,
Paweł Zalewski, Justyna Szymańska, Agnieszka Pawlak, Jan Pawlikowski
Chair and Department of Laser therapy and Physiotherapy, The Ludwik Rydygier Collegium Medicum in Bydgoszcz, The Nicolaus Copernicus University in Toruń, ul. M. Sklodowskiej-Curie 9, 85-094 Bydgoszcz, phone +48 (0) 52 585 34 85, e-mail: kizterfiz@cm.umk.pl
Abstract
Thermal long term low-intensity stimulus through the thermoregulation mechanisms influences blood circulation,
causing dilatation of blood vessels; arterial capillary, arteriole, skin and sub skin veins, opening of closed in normal
circumstances capillaries. Local hyperemia of skin is observed. Metabolism and a diffusion through the capillaries
increases. Parasympathetic nervous system is stimulated, what influences internal organs and a circulatory system,
leading to body relaxation and good mood. A little amount of heat may stimulate immunological reactions,
whereas too much heat inhibits this response. The aim of this work was to evaluate the fluctuations of skin temperature
in some points of foot, shank and thigh after biothermal inlay application. This biothermal inlay has a specific
screen property. The tests were conducted in four groups of subjects: healthy, paraplegic and tetraplegic, with circulatory
problems in lower limbs and placebo. We observed the increase in skin temperature in all groups, except placebo,
however especially in the healthy subjects. "Warm leg signs", were observed, especially in patients with diabetes.
Key words: thermal stimulus, microcirculation, skin temperature measurement
Introduction
Bio-thermal inserts used as footwear inserts perform a function of screening thermal energy of feet. By reflecting not dispersing heat they influence thermoregulation processes in our bodies, mainly by influence of temperature on microcirculation. The aim of these inserts is to increase body temperature and improve blood circulation. As a result of interaction between the foot and the screen a patient can feel a thermal effect after some time (5 to 15 minutes) and sometimes a tingling sensation effect. The inserts give a thermal stimulus of low intensity and a long-term effect [1].
Tests conducted in a Laboratory of Biotronics and Electro photography in Kielce showed that, due to the material of which the inserts are made, they have specific properties energostimulating energetic field of our organism (fig. 1). Direction of changes of these fields depends on individual features of the examined people; approximately 80% of the examined people positively reacted to stimulation. It was shown by filling out of the energetic fields of their feet [2].
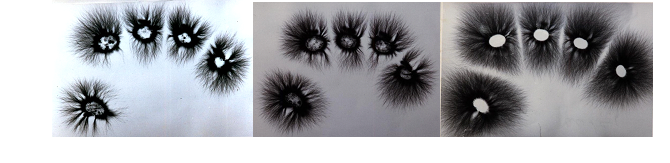
Fig. 1 Evaluation of energetic field of toes: a) after 15 minutes on felt, b) after 15 minutes on a rubber insert, 3)after 15 minutes on a thermal insert (by courtesy of the PIOKAL company)
By reflected thermal energy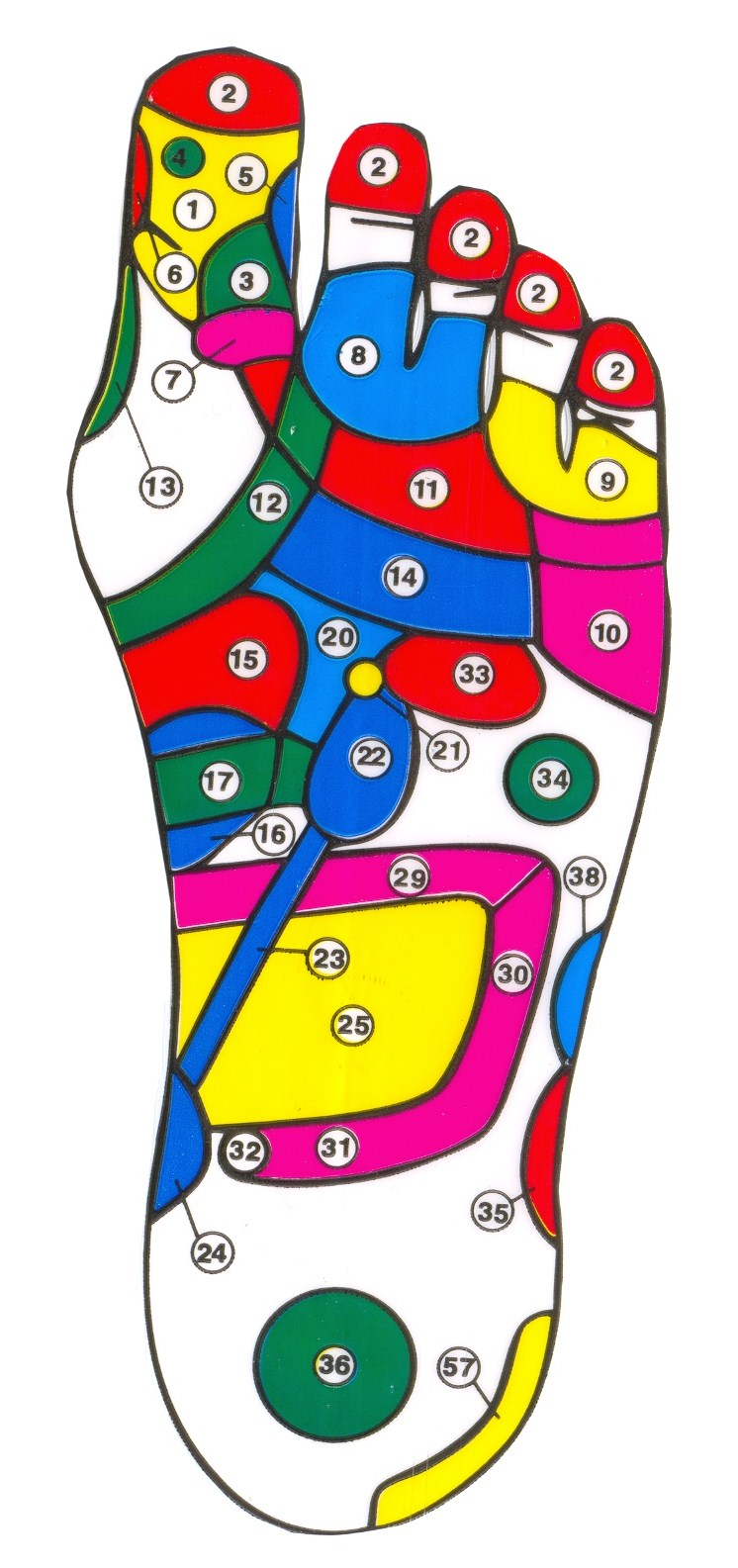 , the inserts have positive influence on receptors on the foot skin (fig 2).
, the inserts have positive influence on receptors on the foot skin (fig 2).
The aim
A research team, after an analysis of literature on help and influence on thermoregulation mechanisms of an organism with the use of physical therapeutic agents, assumed that the research project is to give answer to the following questions:
Fig. 2 Receptors of the left foot (with the PIOKAL company’s agreement)

Fig. 3 the Piokal thermal inserts
- Does the application of the Piokal thermal inserts influence these changes in lower extremities measured in particular points?
- If thermal inserts influence thermoregulation mechanisms in lower extremities, does the temperature change depend on a disease entity?
Material and methods
Research on influence of thermal inserts (fig. 3) on skin temperature of lower extremities was conducted in Chair and Department of Laser therapy and Physiotherapy, Collegium Medicum the Nicolaus Copernicus University (NCU) in Bydgoszcz.
The research material consisted of four groups: three research groups and one control group – placebo. The research groups had the following characteristics:
- group I (research) – consisted of only healthy people declaring no chronic health ailments;
- group II (research) – consisted of people who were patients of the Outpatient Rehabilitation Clinic and of Rehabilitation Teaching Hospital at the NCU in Bydgoszcz; these people had been treated due to chronic dysfunction in the spinal cord and lower part of the spine, of different etiology, with dysaesthesia and circulatory disturbances in lower extremities;
- group III (research) – also consisted of people who were patients of the Outpatient Rehabilitation Clinic and of Rehabilitation Teaching Hospital at the NCU in Bydgoszcz with chronic peripheral circulatory failure in lower extremities;
- control group (placebo) - consisted of only healthy people just like group I, however, placebo inserts instead of therapeutic inserts were applied in this group.
The research methodology based on measurement of temperature on the skin surface in defined points of the body. They were always the same points of measurement in each research group and in the placebo group.
The following measurement points were selected on the skin surface:
- dorsal surface of a foot, just above the dorsal artery of the foot;
- lateral and medial belly of gastrocnemius muscle;
- 15 cm above the knee joint, above the straight muscle of the thigh.
The measurements were done on both sides with the use of a laser temperature measuring instrument of the Raytek Company. The measurements were done in the environment of permanent temperature in order to eliminate the influence of external temperature on the thermoregulation processes. The measurements were done before wearing of therapeutic inserts, and then the inserts were worn for approx. 30-40 min, and after that time next measurement was done and registered in the results table. Therapeutic inserts were applied in research groups, however, in the placebo group identically looking inserts were used but they were made of neutral material. All inserts were sawn up in the same fabric.
Results
Results obtained in respective groups are presented in tables 2-4. Measurements done on healthy individuals are presented in table 1.
In the first group of healthy individuals without dysaesthesia or dysfunction of peripheral circulation, an increase of skin temperature in all tested points was shown, especially in the range of a foot and a shank. These people reported a subjective feeling of warmth after about 5-10 minutes of putting on the inserts, sometimes the tingling sensation and heaviness of feet.
Table 2 presents the results of measurements done on patients with spinal cord injury.
The increase of temperature in all tested points was observed in the group of patients after spinal cord injuries, with dysaesthesia and circulatory disturbances in the lower extremities due to neurogenic disturbances, but the increase of temperature was lower than in the group of healthy people, however, it could be compared in the same proportion. These patients did not report subjective feelings due to dysaesthesia.
Table 3 shows results of measurements done on patients with peripheral circulatory disturbances in the lower extremities.
Measurements also showed increase of temperature on the skin surface in proportion in all points, but due to disturbances in peripheral circulation which caused disorder in thermoregulation processes; these changes of temperature were smaller.
Table 4 presents results of temperature measurements after putting on the placebo inserts – rubber sewn up in fabric.
Graphs show comparative analysis of the obtained temperature measurements in individual points. The average change of temperature within an individual measurement point in respective groups – [0C] graph 4,5,6,7.
The difference of average temperature changes in respective research groups in comparison with the placebo group was analyzed - [0C], what is shown on graphs 8, 9, 10.
Table 1 Results of measurements obtained in the research group I
|
Anatomical location of the measurement point |
Number of temperature measurements [n] |
Average temp. before application of inserts [0C] |
Average temp. after 30- 40 min [0C] |
Average change of temperature [0C] |
|
dorsal surface of a foot |
100 |
32.47 |
33.69 |
1.22 |
|
medial belly |
100 |
32.82 |
33.50 |
0.68 |
|
lateral belly |
100 |
32.76 |
33.46 |
0.70 |
|
15 cm above the knee joint |
100 |
33.03 |
33.35 |
0.32 |
Table 2 Results of measurements obtained in the research group II
|
Anatomical location of the measurement point |
Number of temperature measurements [n] |
Average temp. before application of inserts [0C] |
Average temp. after 30 - 40 min [0C] |
Average change of temperature [0C] |
|
dorsal surface of a foot |
50 |
31.86 |
32.55 |
0.68 |
|
medial belly |
50 |
33.77 |
34.31 |
0.53 |
|
lateral belly |
50 |
33.72 |
34.26 |
0.54 |
|
15 cm above the knee joint |
50 |
33.28 |
33.50 |
0.22 |
Table 3 Results of measurements obtained in the research group III
|
Anatomical location of the measurement point |
Number of temperature measurements [n] |
Average temp. before application of inserts [0C] |
Average temp. after 30 - 40 min [0C] |
Average change of temperature [0C] |
|
dorsal surface of a foot |
35 |
29.93 |
30.32 |
0.39 |
|
medial belly |
35 |
30.02 |
30.61 |
0.41 |
|
lateral belly |
35 |
30.14 |
30.59 |
0.46 |
|
15 cm above the knee joint |
35 |
30.37 |
30.48 |
0.11 |
Table 2 Results of measurements obtained in the placebo group
|
Anatomical location of the measurement point |
Number of temperature measurements [n] |
Average temp. before application of inserts [0C] |
Average temp. after 30 - 40 min [0C] |
Average change of temperature [0C] |
|
dorsal surface of a foot |
53 |
31.21 |
31.43 |
0.22 |
|
medial belly |
53 |
32.42 |
32.56 |
0.15 |
|
lateral belly |
53 |
32.69 |
32.89 |
0.20 |
|
15 cm above the knee joint |
53 |
32.31 |
32.34 |
0.03 |
Discussion
As the presented measurements showed, application of thermal screening inserts for feet for 30 – 40 minutes caused increase of temperature on the surface of the skin on a foot, a shank and above knees. These changes were the highest among healthy people ,obviously due to properly functioning thermoregulation mechanisms. After only such a short time of application the temperature increased especially within a foot, then a shank and in the lowest extent within a thigh. It is probable that after a longer application these changes would be more visible.
Comparative increase of skin temperature was also observed in people who could not state subjective feeling of warmth – patients after spinal cord injury with dysaesthesia. These changes were less visible due to abnormal nerve supply of microcirculation vessels in feet. However, application of inserts also brings effects in this group of patients.
Most subjective sensations were reported by patients with disorders of peripheral circulation within the lower extremities. Despite damage of microcirculation within the lower extremities, increase of temperature was also reported by this group of patients; it was lower within feet and higher within shanks – it is probable that the thermoregulation mechanisms act more efficiently to the level of a shank. The “warm feet” sensations were reported by these patients.
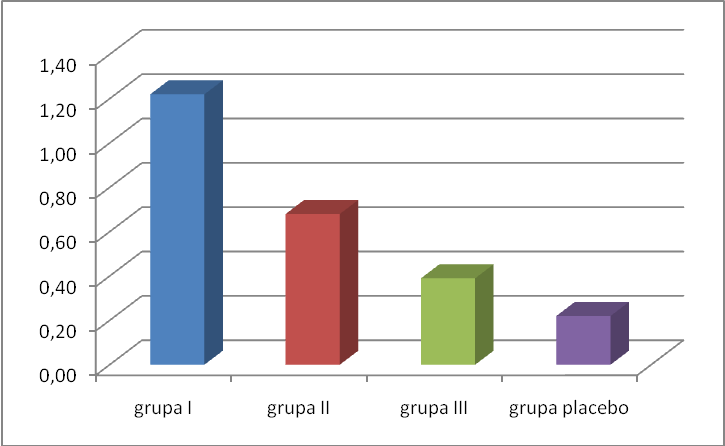
Graph 4 Average change of temperature in all research groups and in the placebo group within dorsal surface of a foot
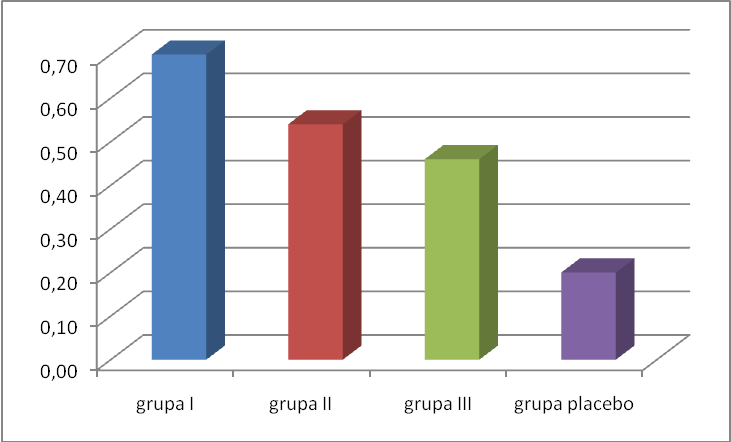
Graph 5 Average change of temperature in all research groups and in the placebo group within lateral belly of gastrocnemius muscle

Graph 6 Average change of temperature in all research groups and in the placebo group within medial belly of gastrocnemius muscle
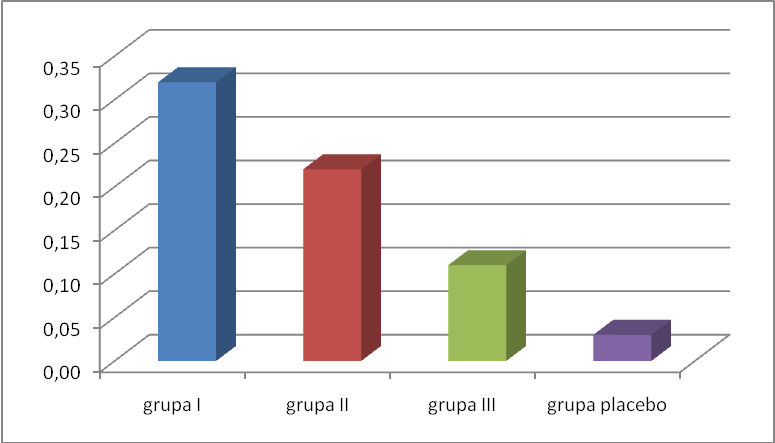
Graph 7 Average change of temperature in all research groups and in the placebo group 15 cm above the knee joint, above the straight muscle of the thigh
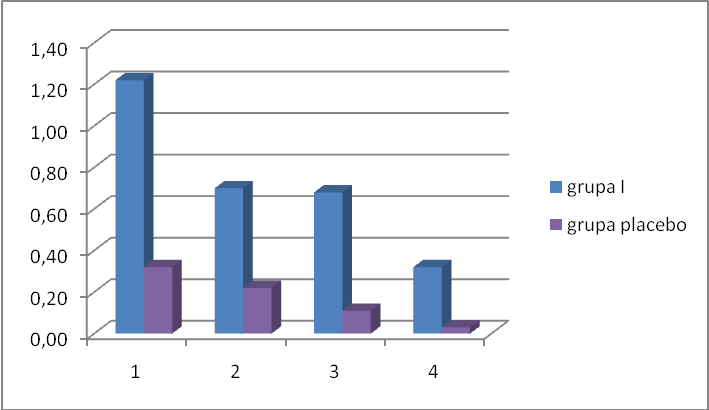
Graph 8 Comparison of average changes of temperature in individual measurement points in research group I, in reference to the placebo group
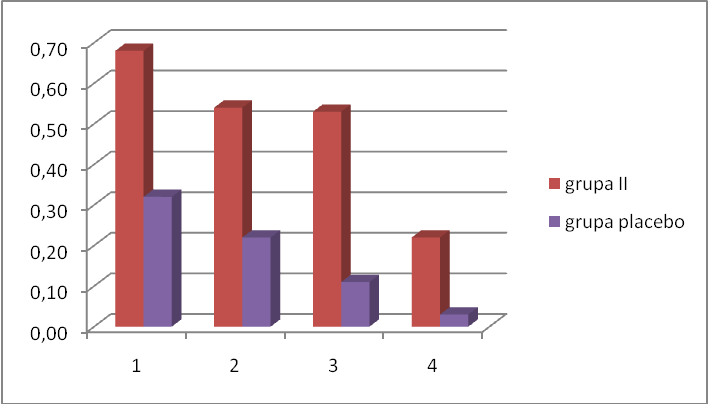
Graph 9 Comparison of average changes of temperature in individual measurement points in research group II, in reference to the placebo group
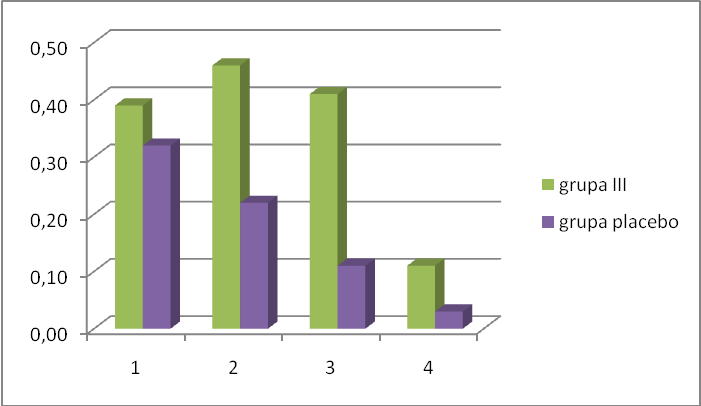
Graph 9 Comparison of average changes of temperature in individual measurement points in research group III, in reference to the placebo group
These sensations were stronger when patients had worn the inserts longer. It is recommended to use the inserts for a longer period of time for this group of patients.
It is known that blood vessels: arterioles, capillary vessels, skin and panniculs veins get expanded and capillaries inactive in normal temperature are opened under the influence of a weak, long-lasting thermal stimulus. These changes cause considerable increase of blood supply to skin. Diffusion through the vascular wall of capillaries is increased and metabolism is improved. It causes stimulation of parasympathetic part of the nervous system, which influences internal organs and respiratory and circulatory systems and also gives the feeling of wellbeing and relaxation. Sudden action of a large dose of warmth leads in the first moment to an adverse reaction – contraction of blood vessels [1].
The volume of the stimulus, time of action, dynamics of its influence, individual features, coexisting illnesses are important for these changes.
In case of thermal inserts the acting stimulus is long-lasting and of low intensity. Influence of these inserts on foot receptors gives additional effect as foot receptors according to the Chinese medicine are considered to be biologically active points connected with channels in which life energy circulates. These channels join our largest organ the skin with the interior of the body [3]. This is probably the source, as well as the influence of the thermal stimulus through the sympathetic system, of positive effects of thermal inserts described by Russian researchers in different disease entities – diabetes, bronchial asthma (research done by prof Danilow from Minsk) [4].
Results obtained by us are comparable with research by Mazanik done on patients with circulatory disturbances within the lower extremities.
Conclusions
The following conclusions were drawn after analysis of the collected material:
- Application of thermal inserts results in increase of skin temperature within a foot, a shank and a thigh in comparison with the placebo group.
- The highest increase was observed in a group of healthy volunteers, without disturbances in blood circulation within the lower extremities.
- Lower increase was reported in patients after spinal cord injury.
- The increase of temperature in a shank was higher than in a foot in patients with dysfunction of circulation within lower extremities; it was probably due to higher intensification of changes within feet. It would indicate that the thermoregulation mechanism after application of inserts is of a reflex character.
- The highest subjective effect of “warm feet” was reported by patients with disturbed microcirculation in the course of diabetes.
- The time of application should be longer for patients with disturbances of peripheral circulation in order to achieve results similar to those achieved in a group of healthy people.
Literature
- G. Straburzyński, A. Straburzyńska-Lupa: Physical Medicine, PZWL Medical Publishing Company, Warsaw 1997, 2000.
- Assessment done by Laboratory of Biotronics and Electrophotography, PTP Department in Kielce, 1994.
- Z. Garnuszewski: A Renaissance of Acupuncture, Sport and Tourism Publishing Company, Warszawa 1988.
- I.P. Danilow: Issledowaniia promienienia stimuliatorow PIOKAL pri bronchialnoj astmie, artymiach i diabeticzeskoj stopie. Science and Research Institute of Hematology and Transfusiology, Minsk 1996.
- L. Mazanik, A.A. Martynowicz, E.G. Slipczenko: Wlijanie bioenergotiermiczeskich wkladisziej PIOKAL na termograficzeskie pokazateli cton pri kosudistych zabolewaniach nizszych koniecznostiei, Medicina, 2002, 3: pp 33-35.
received: 27.07.2007
accepted: 29.08.2007
__________________________________________________________________________________________________________________________
Positive effects of bio-thermal inserts are confirmed by the scientific research conducted as part of scientific and research activities of Ludwik Rydygier Collegium Medicum at the Faculty and Institute of Low Level Laser Therapy and Physiotherapy in Bydgoszcz.
Research project title: "The evaluation of skin temperature variability in the area of lower limbs after the application of bio-thermal inserts."
The results: The inserts are a support therapeutic agent for persons with thermoregulation disorders. The purpose of bio-thermal inserts is to elevate body temperature and improve blood circulation. The inserts give an effect of "warm feet" to people with micro-circulatory disorders in the course of diabetes and peripheral atheromatosis.
The effectiveness of the bio-thermal inserts was also documented by the Laboratory of Biotronics and Electrophotography in Kielce. The research proved that the inserts have specific qualities stimulating the energy field of our organism. The direction of changes of these fields depends on the individual features of the test subjects. Approximately 80% of the test subjects reacted positively to stimulation. It was visible because their energy fields increased and filled out.
Evaluation of the energy field of toes: a) after 15 minutes on a felt insert, b) after 15 minutes on a rubber insert, 3) after 15 minutes on a bio-thermal insert
Positive changes in the appearance of the energy fields indicate the initiation of healing processes.